

The deltoid muscle is vital for shoulder movement and stability. This guide covers its anatomy, functions, common injuries, and exercises for strengthening and rehabilitation.
Key Takeaways
The deltoid muscle has three parts-anterior, middle, and posterior-each responsible for different shoulder movements like flexion, abduction, and rotation.
Maintaining deltoid strength is crucial for shoulder stability and function; injuries can lead to significant weakness and limited range of motion.
Targeted exercises, such as dumbbell raises and military presses, are effective for strengthening the deltoid and enhancing shoulder performance after injury.
Anatomy of the Deltoid Muscle
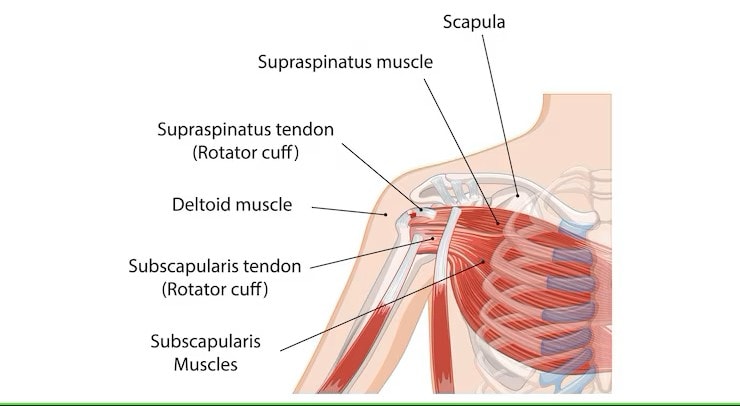
The deltoid muscle, named for its triangular shape, is a prominent shoulder muscle of the shoulder joint. With its pennate fiber arrangement, the deltoid muscle consists of three distinct sets of fibers: the anterior, middle, and posterior. This muscle lies superficial to the fascia, platysma, and skin, overlapping with critical muscles like the rotator cuff, pectoralis major, biceps, and triceps.
Positioned just beneath the fascia, platysma muscle, and skin, the deltoid muscle is crucial for shoulder movement and stability. It covers important neurovascular structures, including the axillary nerve and the anterior and posterior circumflex humeral vessels, making it a crucial muscle for both movement and protection.
Knowing the deltoid muscle’s anatomy highlights its function and underscores the need to maintain its strength and health. Besides being a powerhouse for movement, it also shields vital structures in the shoulder.
Deltoid Muscle Diagram
Deltoid Muscle Parts
The deltoid muscle is divided into three parts: the anterior (clavicular), middle (acromial), and posterior (scapular spinal). Each part originates from a different area. The anterior deltoid starts from the upper surface of the clavicle, the middle part from the acromion, and the posterior fibers from the spine of the scapula.
All three parts of the deltoid muscle converge at the deltoid tuberosity on the humerus, facilitating a wide range of shoulder movements. This triad of muscle fibers works together to perform complex shoulder actions, making the deltoid a versatile and crucial muscle for upper limb mobility.
Anterior Deltoid
The anterior deltoid originates from the lateral third of the clavicle and inserts at the deltoid tuberosity of the humerus. This part of the deltoid muscle is primarily responsible for shoulder flexion and medial rotation, playing a significant role in raising the arm forward.
Reaching above shoulder and upper height heavily relies on the anterior deltoid. Injury to this muscle can cause difficulties in overhead movements, emphasizing its role in daily activities and sports.
Middle Deltoid
The middle deltoid, also known as the lateral deltoid, originates from the acromion of the scapula and shares the common insertion point at the deltoid tuberosity on the humerus. This part of the deltoid muscle is primarily responsible for arm abduction, allowing the arm to lift sideways away from the body.
The middle deltoid stabilizes the shoulder joint during arm movements, ensuring smooth and controlled abduction. Its strength and functionality are essential for activities that require lifting objects or performing lateral movements.
Posterior Deltoid
The posterior deltoid originates from the lateral third of the spine of the scapula and inserts at the deltoid tuberosity on the humerus, similar to the other parts of the deltoid. This part of the deltoid is primarily responsible for lateral rotation and extension of the arm, contributing to movements that involve lifting the arm backward.
Weakness in the posterior deltoid can greatly affect shoulder stability and movement, particularly in overhead actions. Its role in shoulder extension and external rotation is vital for various athletic and daily activities.
Deltoid Muscle Function
The deltoid muscle drives shoulder movements, working in coordination with other shoulder muscles. It aids in arm abduction, flexion, extension, and rotation, ensuring a wide range of motion and stability.
This multifaceted muscle is vital for both everyday tasks and athletic activities.
Shoulder Abduction
A primary function of the deltoid muscle is shoulder abduction, lifting the arm laterally away from the body. All three heads of the deltoid muscle work together to facilitate this movement, allowing for arm elevation in different directions, including front, side, and back.
In shoulder abduction, the deltoid stabilizes the humeral head within the glenoid cavity, preventing dislocation. Weakness or injury to the deltoid can significantly reduce the ability to perform shoulder abduction, impacting daily activities that involve lifting or carrying objects.
Shoulder Flexion and Extension
The deltoid flexes the arm forward and extends it backward, enabling a wide range of motion. The anterior fibers of the deltoid facilitate shoulder flexion, while the posterior fibers contribute to shoulder extension.
In shoulder flexion, the anterior deltoid raises the arm forward, while the posterior deltoid moves it backward during extension. This coordination ensures smooth and controlled shoulder movements, essential for various activities.
Stabilization of the Shoulder Joint
The deltoid stabilizes the shoulder joint during arm movements, preventing dislocations. It maintains the humeral head’s position within the glenoid cavity, providing dynamic stability.
This stabilization is crucial, especially when the shoulder joint faces instability.
Innervation and Blood Supply
The axillary nerve arises from the C5 and C6 cervical nerves and innervates the deltoid muscle. Branches of the axillary artery and the posterior circumflex humeral artery supply the deltoid muscle with essential nutrients and oxygen.
Function of the Deltoid Muscle
As a primary mover, the deltoid muscle facilitates shoulder abduction, flexion, extension, and rotation, contributing to various arm activities. It collaborates with the rotator cuff muscles to stabilize the glenohumeral joint, enabling dynamic movements.
Dynamic Shoulder Abduction
Testing deltoid function involves positioning the arm beyond 15 degrees of abduction and applying resistance. During abduction, proper deltoid function is indicated by muscle contraction felt near the acromion of the scapula.
In dynamic shoulder abduction, inability to initiate abduction up to 15 degrees may suggest involvement of the supraspinatus muscle, which works with the deltoid. The deltoid muscle is essential for dynamic shoulder abduction, enabling the arm to move away from the body.
Clinical Considerations
Deltoid muscle injuries are classified into three grades based on severity, affecting functionality and pain levels differently.
Often resulting from acute trauma or chronic overuse, these injuries lead to symptoms like:
pain
weakness
swelling
limited range of motion
Axillary Nerve Injury
Axillary nerve injury can significantly impair deltoid function, causing:
muscle atrophy
weakness
loss of muscle tone
shoulder flattening
loss of sensation
Humeral fractures, glenohumeral dislocations, and improper crutch use commonly cause axillary nerve palsy. Such injuries can lead to significant shoulder weakness and impaired movement.
Subacromial/Subdeltoid Bursitis
The subacromial/subdeltoid bursa lies beneath the deltoid muscle, positioned between the acromion and the supraspinatus tendon. Repetitive pinching between the acromion and the greater tubercle of the humerus causes subacromial bursitis, leading to irritation and swelling of the bursa.
Irritation can lead to the bursa becoming distended. This distension may result in pain beneath the deltoid muscle. This condition can cause difficulties in arm movement, especially when lifting overhead due to inflammation.
Exercises for Deltoid Muscle Strengthening
Post-injury deltoid strengthening can be achieved through targeted exercises under physiotherapy supervision. Such exercises are crucial for enhancing shoulder stability and functionality.
Deltoid Muscle Strengthening Exercise Diagram
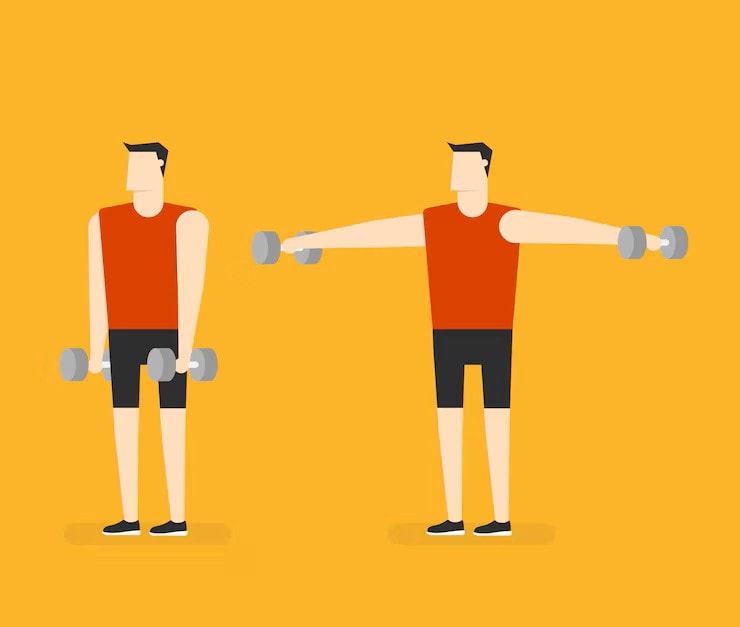
Shoulder Abduction Exercises
Dumbbell lateral raises target the deltoid muscle, improving strength through shoulder abduction. Seated dumbbell shoulder presses enhance overhead strength and stability for the deltoid muscles.
Regular practice of these shoulder abduction exercises leads to significant improvements in deltoid strength and overall shoulder functionality.
Flexion and Extension Workouts
The military press targets the anterior deltoids through shoulder flexion. This exercise is key for developing the anterior deltoids, supporting overhead activities.
Rehabilitation and Recovery
Recovery from axillary nerve injury varies, typically taking between 3 to 12 months.
Deltoid strengthening exercises enhance shoulder stability and posture, reducing injury risk.
Post-Surgery Recovery
Patients can see noticeable improvements in deltoid function within 6 to 12 weeks post-surgery with consistent exercises. Post-surgical recovery for the deltoid may involve assisted exercises to gradually restore mobility and strength.
Using pain as a guide during rehabilitation exercises is important to avoid overexertion and ensure proper healing. Strengthening internal and external rotation exercises are crucial in the later stages of recovery to regain shoulder function.
Relation to Other Shoulder Muscles
The deltoid assists in flexing the arm, moving it forward into an overhead position. It also extends the arm, moving it backward behind the body. The deltoid stabilizes the shoulder joint, preventing dislocations when lifting the arms.
Deltoid and Rotator Cuff Interaction
The deltoid facilitates arm abduction, flexion, extension, and rotation, playing a crucial role in shoulder movement. Testing deltoid function requires raising the arm beyond 15 degrees of abduction and applying resistance. Failure to initiate arm abduction indicates a lack of involvement from the supraspinatus muscle, essential for the initial 15 degrees of movement.
The anterior and posterior parts of the deltoid converge onto the inserting tendon, reinforcing shoulder stability when interacting with the rotator cuff. This interaction ensures smooth movement and stability of the shoulder joint during various activities, emphasizing the importance of both muscle groups working together.
Common Injuries and Treatments
Deltoid muscle problems often stem from repetitive overhead activities, increasing the risk of injuries in athletes. Such injuries can lead to complications like pain, weakness, and impaired movement.
Initial treatments typically involve rest, ice, and heat application to minimize pain and swelling.
Rotator Cuff Tears
Rotator cuff tears can significantly affect deltoid function and may require surgical intervention for rotator cuff repairs. Such tears can lead to significant dysfunction in the deltoid, affecting shoulder stability and movement. The deltoid often compensates for rotator cuff injuries, leading to additional strain and dysfunction.
Symptoms of rotator cuff tears may include shoulder pain, restricted motion, and weakness, impacting deltoid function. Early diagnosis and treatment are crucial to prevent further complications and ensure proper healing, particularly in the context of rotator cuff tear progression.
Shoulder impingement syndrome
Shoulder impingement syndrome occurs when the rotator cuff tendon is compressed between the acromion and the humeral head, often due to muscle imbalances. The deltoid can become stronger than the rotator cuff, leading to improper joint mechanics and potential impingement. Symptoms include pain during overhead activities and discomfort that may worsen at night.
Preventing shoulder impingement involves balancing strength training between the deltoid and rotator cuff muscles. Ensuring both muscle groups are equally strong and flexible helps maintain proper shoulder mechanics and reduces the risk of impingement.
Deltoid strains
Deltoid strains result from excessive use or trauma, often presenting as pain in different parts of the shoulder. Such strains often occur due to muscle overuse without sufficient rest, leading to symptoms like pain, swelling, and reduced function. They are classified into three grades based on severity, with Grade 1 being mild and Grade 3 indicating complete muscle tears.
Initial treatment for mild strains typically involves the P.R.I.C.E. method, focusing on protection, rest, ice, compression, and elevation. Recovery times vary, potentially spanning from a couple of days for mild cases to several weeks for severe injuries.
Physical therapy is often recommended for more severe strains to regain motion and strength post-injury.



