

The tibia and fibula anatomy refers to the two long bones in your lower leg. The tibia, also known as the shin bone, bears most of your weight and connects your knee to your ankle. The fibula, positioned beside the tibia, mainly serves as a site for muscle attachment. If you’re looking to understand how these bones support movement and weight, this guide will break down their structure, function, key joints, and common related conditions.
Key Takeaways
The tibia, or shin bone, is crucial for weight-bearing and movement, while the fibula supports muscle attachment and stability.
Both bones play vital roles in major joints like the knee and ankle, with the tibia contributing to weight distribution and the fibula adding structural support.
Common injuries include fractures to the tibia and fibula, often requiring treatments ranging from immobilization to surgical interventions, with a focus on rehabilitation for recovery.
Tibia and Fibula Anatomy
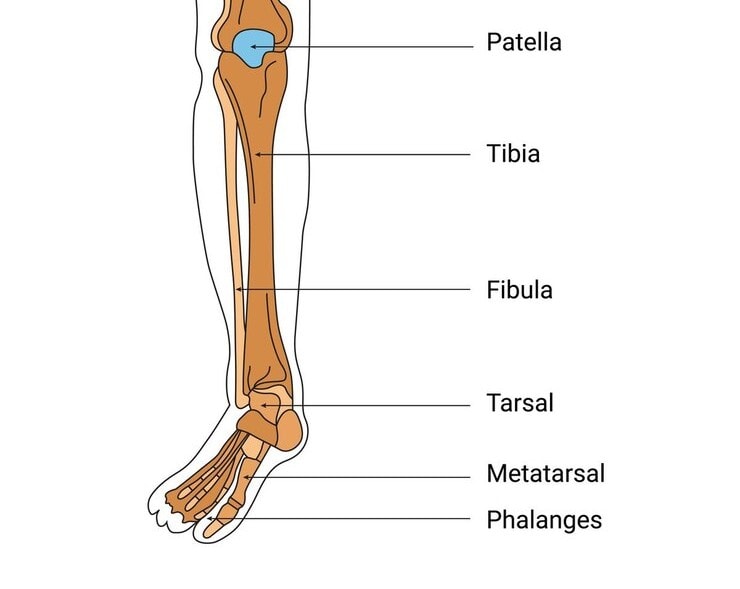
The tibia, also known as the shin bone, is the second longest bone in the human body, playing a crucial role in weight-bearing and movement. It runs from below the knee to the ankle, positioned medially to the fibula. The fibula, a slender bone located laterally to the tibia, primarily serves as a site for muscle attachment rather than weight-bearing.
Together, these two bones form the structural foundation of the lower leg and the calf bone, enabling us to stand, walk, and perform a myriad of activities.
Tibia and Fibula Diagram
Detailed Anatomy of the Tibia
The tibia is divided into three main parts: the proximal end, the body (or shaft), and the distal end. Each section plays a unique role in the bone’s overall function. The proximal tibia articulates with the femur at the knee joint, providing stability and movement.
The tibial shaft is designed for strength and weight-bearing, while the distal tibia forms part of the ankle joint, crucial for mobility and balance.
Proximal Tibia
The proximal end of the tibia is characterized by two important landmarks: the medial and lateral condyles. These condyles are essential for the articulation with the femoral condyles, forming the knee joint. The superior surface of the medial condyle is round and somewhat concave, perfectly designed to fit into the medial femoral condyle, ensuring stability during movement. On either side of the intercondylar eminence, the medial and lateral intercondylar tubercles serve as crucial projections for ligament attachment, further stabilizing the knee.
This region is not just about stability; it’s also about facilitating movement. The articulation between the tibial condyles and the femoral condyles is vital for knee function, allowing flexion and extension. This interaction is fundamental to activities ranging from walking to running, highlighting the importance of the proximal tibia in our daily lives.
Tibial Shaft
The tibial shaft, or body, is prism-shaped, contributing to its strength and functionality as a weight-bearing bone. One notable feature is the anterior border, which is easily palpable and serves as a landmark for medical examinations. Unlike other parts of the tibia, the medial surface is subcutaneous, meaning it has no muscle attachments, making it unique in its exposure and clinical significance.
The tibial shaft serves as an anchor for several key muscles, including:
sartorius
gracilis
quadriceps femoris
semimembranosus
semitendinosus
popliteus
These muscles play critical roles in movements such as knee flexion, extension, and stabilization, emphasizing the tibial shaft’s importance beyond mere structural support.
Distal Tibia
The distal tibia is easily recognizable by its rectangular cross-section shape. One of its most prominent features is the medial malleolus, a bony projection that plays a crucial role in the formation of the ankle joint. This structure articulates with the tarsal bones, providing stability and support for the ankle, essential for activities such as walking and running.
Key Joints Involving the Tibia and Fibula
The tibia and fibula are integral to major joints, including the knee joint and ankle joint. These bones work together to provide stability and facilitate movement. The medial and lateral malleoli are particularly important for the stability of the ankle joint, highlighting the significance of these bones in our daily activities.
Knee Joint
The knee joint is formed by the articulation between the tibial and femoral condyles, creating a stable surface for movement. The medial and lateral condyles of the tibia, known as the tibial plateau, play a crucial role in knee stability and function. This articulation allows for the flexion and extension necessary for activities such as walking, running, and jumping.
Ankle Joint
The ankle joint is formed by the distal ends of the tibia and fibula, which articulate with the talus. The lateral malleolus, located at the fibula’s distal end, is more pronounced than the medial malleolus and plays a key role in stabilizing the ankle joints. This bony prominence helps prevent excessive lateral movements, reducing the risk of injuries.
Fibula fractures often accompany ankle injuries and can result from direct trauma or twisting motions. These fractures can lead to complications such as instability of the ankle joint, emphasizing the importance of the fibula in maintaining ankle stability.
The distal tibiofibular joint, formed by the tibia and fibula, further supports the ankle joint.
Interosseous Membrane
The interosseous membrane is a fibrous connection that links the shafts of the tibia and fibula, playing a crucial role in stability during movement. It aids in weight distribution between the two bones and helps absorb forces during weight-bearing activities, ensuring the leg functions smoothly.
Muscle Attachments on the Tibia and Fibula
Muscle attachments on the tibia and fibula are vital for movement and stability. While the fibula primarily serves as a site for muscle attachment, the tibia also plays a role in anchoring several key muscles. These muscles are grouped into the anterior and posterior compartments, each with specific functions and innervations.
Anterior Compartment Muscles
The anterior compartment of the leg contains muscles primarily responsible for dorsiflexion of the foot. This includes the tibialis anterior, extensor hallucis longus, and fibularis tertius, all innervated by the deep fibular nerve.
The tibialis anterior, located on the anterior surface of the leg, is crucial for dorsiflexing the foot and inverting it, playing a significant role in walking and running.
Posterior Compartment Muscles
The posterior compartment of the leg houses key muscles such as the tibialis posterior, flexor digitorum longus, and soleus. These muscles are essential for plantarflexion and stabilization of the foot.
The compartment is divided into superficial and deep layers, each containing distinct muscle groups that contribute to different aspects of movement and support.
Common Conditions Affecting the Tibia and Fibula
Common conditions affecting the tibia and fibula include fractures, osteoporosis, and Paget’s disease. Osteoporosis leads to weakened bones, increasing the risk of fractures, particularly in older adults and females. Paget’s disease causes chronic changes in bone structure, often seen in individuals over 50.
These conditions can significantly impact the function and health of the tibia and fibula, necessitating proper diagnosis and treatment.
Tibia Fractures
The tibial body is the most vulnerable part of the tibia to fractures, often resulting from high-impact activities or accidents. A tibial plateau fracture, involving the proximal tibia, is a common injury from serious impacts. Severe tibial fractures may require surgical intervention to ensure proper healing and restore function.
Fibula Fractures
Fibula fractures can occur due to trauma or hyperextended knees. Common types include spiral fractures from forced external rotation and transverse fracture from twisting the foot outwards. An avulsion fracture, caused by sudden muscle or ligament jerks, is another type of fibula fracture.
Treatment typically involves immobilization with a splint or cast, and in some cases, surgery may be necessary.
Diagnostic Tests for Tibia and Fibula Issues
Diagnostic tests for the tibia and fibula include bone density tests, such as DEXA scans, which measure bone strength and identify bone loss. These tests are crucial for early detection of osteoporosis, allowing for proactive management of bone health.
Additionally, X-rays are commonly used to diagnose fractures, while MRI and CT scans provide detailed images to assess damage to surrounding muscles and ligaments.
Treatment Options for Tibia and Fibula Injuries
Treatment options for tibia and fibula injuries vary depending on the severity and type of fracture. Non-displaced fractures can often be treated with immobilization using a splint or cast. However, severe fractures may require surgical intervention, such as closed reduction to realign the bones without surgery or internal fixation to secure the bones in place for healing. In some cases, external fixation might be necessary, where screws are placed inside the bone and connected to an external device.
Post-surgical rehabilitation is critical for ensuring proper recovery and function of the tibia and fibula. Physical therapy is essential for restoring strength and mobility, helping patients return to their normal activities.
Complications from treatment can include malunion, where bones heal incorrectly, or infection in open fractures, necessitating careful surgical planning and follow-up care.
Surgical Considerations Involving the Tibia and Fibula
Surgeons often use the fibula for bone grafts due to its lighter role in weight-bearing compared to the tibia. The fibula’s sufficient length and vascular supply make it an ideal candidate for reconstruction, facilitating healing.
Surgical procedures involving the tibia and fibula require careful consideration to avoid complications, such as damaging surrounding neurovascular structures. The fibula’s anatomical characteristics play a significant role in these surgical decisions.



