

The clavicle, or collarbone, is a vital part of your body’s skeletal system. It links your shoulder to your chest, allowing arm movement and providing stability. In this article, discover the key roles, structure, and common injuries related to the clavicle.
Key Takeaways
The clavicle connects the axial and appendicular skeletons, playing a crucial role in shoulder mobility and stability.
Clavicle fractures are common injuries, often resulting from falls or impact, particularly during sports, and require proper management for recovery.
The clavicle’s unique anatomy, including key muscle attachments and joint articulations, is essential for arm movement and overall shoulder function.
Clavicle Overview
The clavicle, or collarbone, serves as a vital connection between the axial skeleton and the appendicular skeleton, forming an integral part of the pectoral girdle. This slender, S-shaped bone is unique in its horizontal orientation, making it the only long bone in the body that lies horizontally. The clavicle’s design allows it to absorb and transmit forces from the upper limb to the central skeleton, acting as a strut between the scapula and the sternum.
Its strategic position and structure enable the clavicle to connect the upper limb to the trunk, playing a crucial role in shoulder mobility and stability. The clavicle articulates with the shoulder blade (scapula) and the sternum, forming essential joints that facilitate a range of arm movements. This articulation is key to the clavicle’s function as a supportive structure, maintaining the shoulder’s distance from the thorax and allowing a greater range of motion.
Absorbing and transmitting forces, the clavicle plays a significant role during activities involving the upper limbs, such as lifting, pushing, and pulling. This bone’s structural attributes and its role in connecting major skeletal components underscore its importance in both everyday movements and more strenuous physical activities.
Clavicle Diagram
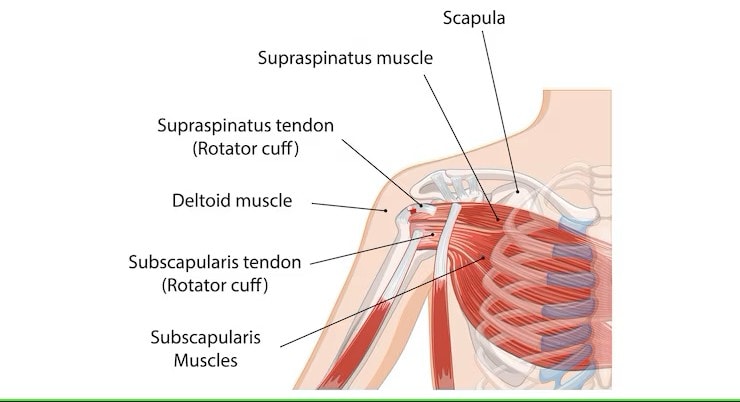
Anatomical Structure of the Clavicle
Delving into the anatomical structure of the clavicle reveals a fascinating blend of form and function. This bone’s unique shape, position, and surface features are all tailored to its roles in movement, muscle attachment, and force transmission.
The clavicle’s horizontal alignment and its connection to the axial skeleton highlight its importance in the broader context of human anatomy.
Bone Structure
The clavicle is a long bone shaped like a sigmoid curve, with a convexity on its medial end and a concavity on its lateral end. This distinctive ‘S’ shape allows the clavicle to function effectively as a strut, maintaining the position of the shoulder blade relative to the sternum. Key anatomical landmarks on the clavicle include the medial sternal end, which articulates with the sternum, and the lateral acromial end, which connects to the scapula.
The clavicle provides distinct attachment sites for muscles like the sternocleidomastoid and pectoralis major, essential for its function. These attachment points are not only essential for muscle function but also for the structural integrity of the clavicle during various movements and activities.
Location and Position
Anatomically, the clavicular head lies horizontally at the base of the neck, positioned between the sternum and the scapula. This location enables the clavicle to act as a strut that keeps the shoulder away from the thorax, thereby allowing a greater range of shoulder motion.
The clavicle’s strategic position also plays a crucial role in shoulder stability and arm movement, making it an indispensable component of the human skeletal system.
Surface Anatomy of the Clavicle
The clavicle can be palpated easily along its entire length, especially at the junctions of the sternal and acromial ends. The sternal end of the clavicle articulates with the manubrium of the sternum, forming the sternoclavicular joint, while the acromial end connects with the acromion of the scapula, forming the acromioclavicular joint. These surface features are not only important for muscle attachment but also for clinical assessments of clavicle injuries.
Important surface features of the clavicle include the conoid tubercle and the costal tuberosity, serving as ligament attachment points. The superior and inferior surface of the clavicle also have distinct anatomical features that are critical for muscle and conoid ligament attachments, contributing to the bone’s overall functionality and stability.
Clavicle Joints
Two primary joints formed by the clavicle-the sternoclavicular joint (SC joint) and the acromioclavicular joint (AC joint)-are essential for connecting the arm to the body, enabling a wide range of shoulder movements while ensuring stability and support.
Sternoclavicular Joint (SC Joint)
Connecting the clavicle to the sternum, the sternoclavicular joint serves as the sole point of attachment between the arm and the torso. This synovial joint allows for various movements, including elevation, depression, and rotation of the shoulder. Strong ligaments, such as the costoclavicular ligament and sternoclavicular ligaments, provide stability and support to the SC joint, preventing dislocation and excessive movement.
The SC joint is crucial for shoulder girdle movement, enabling a range of motions that are essential for daily activities and athletic performance. Ligaments surrounding the SC joint ensure shoulder mobility while maintaining structural integrity and reducing injury risk.
Acromioclavicular Joint (AC Joint)
Linking the acromion of the scapula to the clavicle, the acromioclavicular joint facilitates shoulder mobility. This joint primarily allows for the upward and downward movement of the shoulder, along with some rotational motion. The AC joint is stabilized by the acromioclavicular and coracoclavicular ligaments, which provide both horizontal and vertical support.
The acromioclavicular joint functions primarily to allow gliding movements, enhancing the range of motion for the shoulder complex. This joint’s stability is crucial for maintaining shoulder integrity during various activities, from everyday tasks to high-impact sports.
Muscle Attachments on the Clavicle
Muscle attachments on the clavicle are critical for its function and stability. Acting as an anchor for several major muscles, the clavicle plays essential roles in shoulder and arm movements.
Understanding these attachments helps in recognizing the functional significance of the clavicle in the broader context of the musculoskeletal system.
Muscles Attached to the Clavicle
Several key muscles attach to the clavicle, including the sternocleidomastoid, trapezius, deltoid, subclavius, and pectoralis major. The trapezius muscle connects to the posterior surface of the clavicle, while the deltoid muscle attaches to its anterior surface. The sternocleidomastoid muscle is attached to the superior surface, and the subclavius muscle attaches in a groove on the posterior surface. The pectoralis major muscle is affixed to the anterior surface of the clavicle.
These muscle attachments are essential for the clavicle’s role in movement and stability. Each muscle contributes to different aspects of shoulder and arm function, highlighting the clavicle’s importance in the musculoskeletal system.
Functions of Clavicular Muscle Attachments
Muscles attached to the clavicle stabilize the shoulder girdle and facilitate various arm movements. For instance, the trapezius muscle helps in elevating and rotating the scapula, while the deltoid muscle is crucial for arm abduction. The pectoralis major muscle assists in shoulder flexion, horizontal adduction, and inward rotation of the humerus.
These muscle attachments facilitate movement and help maintain the clavicle’s structural integrity during various activities. By stabilizing the shoulder girdle, these muscles ensure that the clavicle can effectively transmit forces and support a wide range of motions.
Blood Supply to the Clavicle
The blood supply to the clavicle is crucial for its health and function, particularly in the context of injury and healing. Insight into the arterial and venous systems serving the clavicle reveals how this bone maintains its vitality and supports recovery.
Arteries Supplying the Clavicle
The clavicle receives arterial blood supply from several key arteries, including the suprascapular artery, the thoracoacromial artery, and the internal thoracic artery. The internal thoracic artery, which branches from the subclavian artery, contributes to the blood supply of the sternoclavicular joint. These arteries are critical for delivering oxygen and nutrients to the clavicle, supporting its metabolic needs and healing processes.
The thoracoacromial and suprascapular arteries significantly vascularize the clavicle, ensuring adequate blood flow. This robust blood supply is essential for maintaining the health of the clavicle and supporting the recovery from injuries.
Venous Drainage of the Clavicle
Venous drainage of the clavicle is primarily facilitated by the subclavian vein, which collects deoxygenated blood from the clavicle and returns it to the heart. A major vessel, the subclavian vein ensures efficient blood flow and removal of metabolic waste products.
In addition to the subclavian vein, the jugular vein system, including the external jugular vein, also contributes to the venous drainage of the clavicle. These veins help maintain proper blood circulation in the clavicle and surrounding areas, supporting overall vascular health and function.
Nerve Supply to the Clavicle
The nerve supply to the clavicle is essential for its sensation and movement. The clavicle and its joints receive innervation from the subclavian, lateral pectoral, and supraclavicular nerves, which are responsible for transmitting sensory and motor signals.
Nerves Involved
The medial supraclavicular nerve (C3-C4) and the subclavius nerve (C5-C6) specifically innervate the sternoclavicular joint, providing sensory and motor innervation. These nerves are part of the brachial plexus, a complex network of nerves that controls the muscles and sensations in the arm and shoulder.
The acromioclavicular joint is innervated by the supraclavicular and lateral pectoral nerves, ensuring proper sensory feedback and motor control. This intricate nerve supply is crucial for the clavicle’s role in movement and sensation, highlighting the importance of understanding its neurological connections.
Clavicle Anatomy
Clavicle fractures are among the most frequent types of commonly fractured bones, comprising around 5% of all adult fractures. These injuries are common in both children and adults, often resulting from direct impacts or falls where fractures occur.
Types of Clavicle Fractures
Clavicle fractures can be classified based on their location:
Midshaft fractures, which are the most common, occurring in the middle third of the clavicle
Lateral fractures, which occur near the acromial end
Medial fractures, which occur near the sternal end
Comminuted fractures, where the bone breaks into multiple fragments, are also a possibility.
Each type of fracture has its own set of challenges and treatment options. Understanding the specific type and location of a clavicle fracture is crucial for effective management and recovery.
Causes of Clavicle Fractures
Clavicle fractures are often the result of direct impacts, such as those sustained during contact sports or falls. Sports injuries are a common cause, particularly in activities that involve high impact or physical contact. Falls and accidents, where the individual lands on an outstretched arm, are also frequent causes of clavicle fractures.
Birth-related injuries can also lead to clavicle fractures in newborns. These fractures can occur during delivery and require careful management to ensure proper healing.
Treatment and Management of Clavicle Fractures
Treatment for clavicle fractures typically involves conservative methods, such as using a simple arm sling and physical therapy to support healing and restore mobility. However, surgical interventions may be necessary for a displaced clavicle fracture or those with a high risk of neurovascular injury.
Surgical treatment often involves realigning the bone and securing it with metal hardware, such as plates and screws. Physical rehabilitation is also a critical component of the recovery process, helping patients regain strength and function after a clavicular fracture.
Clinical Significance of Clavicle Anatomy
Understanding the clinical significance of clavicle anatomy is crucial for recognizing its role in posture, movement, and injury. The clavicle serves as a critical link between the upper limbs and the axial skeleton, facilitating weight transfer and supporting a wide range of shoulder movements.
Role in Posture and Movement
The clavicle is essential for maintaining posture and enabling shoulder girdle movement. Its stability is vital for the overall function of the shoulder girdle, supporting upper body posture and allowing for a wide range of arm motions.
Impact of Clavicle Injuries on Function
Injuries to the clavicle can lead to significant limitations in overhead activities and overall arm movement. Loss of range of motion and disability in arm movement are common consequences of clavicle injuries, highlighting the importance of proper rehabilitation and therapy.
Effective management and rehabilitation are crucial for restoring function and preventing long-term complications. Understanding the impact of clavicle injuries on function can help guide treatment and recovery strategies.
Medial End
The medial end of the medial clavicle articulates with the manubrium of the sternum at the sternoclavicular joint, forming a critical connection for shoulder stability. This end is connected to the opposite clavicle by the interclavicular ligament, enhancing stability and support.
The medial end of the clavicle undergoes endochondral ossification, a process essential for bone development and growth. Understanding these anatomical features is important for recognizing the medial ends of the clavicle’s role in joint formation and stability.
Shaft
The clavicle shaft consists of:
Two segments: the medial two-thirds and the lateral one-third
Anterior border that uniquely attaches to the pectoralis major muscle
Superior surface associated with the deltoid and trapezius muscles
These muscle attachments are crucial for shoulder movement and stability.
The lateral third of the clavicle is particularly important for muscle attachment, impacting shoulder mechanics and function.
Lateral End
The lateral end of the clavicle is referred to as the acromial end. It connects with the acromion of the scapula, creating the acromioclavicular joint. This joint is essential for arm movement and shoulder stability, allowing for a range of motions that are crucial for daily activities and athletic performance.
The lateral aspect of the clavicle is concave, while the posterior border is convex backward, features that are important for muscle and ligament attachments. Understanding the anatomy of the lateral end is vital for recognizing its role in shoulder mechanics and stability.
Key Functions of the Clavicle
The clavicle enables shoulder movement by acting as a strut that allows the scapula to maintain its position during arm actions. By maintaining a distance between the arm and the thorax, the clavicle facilitates greater shoulder mobility. This bone also plays a protective role for neurovascular structures such as the brachial plexus and subclavian vessels, safeguarding them from injury.
Overall, the clavicle acts as a critical connector between the upper limb and the trunk, supporting both movement and protection. Its unique structure and position make it an indispensable component of the human skeletal system, highlighting its importance in both everyday activities and more strenuous physical tasks.
Common Clavicle Injuries
Clavicle injuries are common and include fractures and acromioclavicular joint injuries. These injuries account for about 10% of all fractures and are a significant concern in shoulder-related issues.
Clavicle Fracture
Clavicle fractures commonly occur by impacts to the shoulder from falling on outstretched arms or a direct hit. A clavicle fracture is most commonly caused by falling onto the shoulder. It can also occur due to landing on an outstretched hand. The middle third of the clavicle is the most common site for clavicular fractures.
Common treatments for a fractured clavicle include surgery to realign and secure the bones. Approximately 5% of adult fractures are due to broken clavicles, highlighting the prevalence and significance of these injuries.
Acromioclavicular Joint Injuries
Injuries to the acromioclavicular joint often result from direct impacts or falls. These injuries are prevalent in contact sports, representing 9% of shoulder girdle injuries.
Understanding and treating AC joint injuries is essential for effective shoulder rehabilitation and maintaining overall shoulder function.
Variations and Anomalies
Variations and anomalies in the clavicle can significantly impact its function. Males typically have longer and thicker clavicles compared to females, and left clavicles are generally longer than the right. The condition known as cleidocranial dysplasia is often marked by underdeveloped or completely missing clavicles, leading to excessive shoulder mobility due to associated muscle defects.
Here are some key points regarding clavicle variations:
Males have a greater degree of curvature in the clavicle than females.
The prevalence of cleidocranial dysplasia is roughly estimated at one in a million, showing no significant difference across races or genders.
Anatomical variations in the supraclavicular nerve can include branches that course beneath the clavicle’s surface.
Recognizing these variations is crucial for identifying potential issues and tailoring treatment approaches to individual needs.
Surgical Considerations for Clavicle Injuries
Surgical considerations for clavicle injuries are essential for effective treatment and recovery. Common management options for a clavicle fracture include conservative treatment like sling immobilization or operative treatment such as open reduction and internal fixation. Surgical intervention is often recommended for fractures that exhibit significant displacement or have a risk of neurovascular injury.
Fixation methods for clavicle fractures include both plates and screws, as well as intramedullary nails. Surgical treatment tends to lead to better recovery times and higher levels of patient satisfaction compared to conservative methods.
Understanding these surgical considerations can help patients and healthcare providers make informed decisions about the best treatment options for clavicle injuries.



