

Skull anatomy examines the structure of the human skull’s 22 bones. This guide explains how these bones protect the brain and form the face. Read on to learn about the skull’s key regions, individual bones, and their functions.
Key Takeaways
The human skull consists of 22 bones, with a primary role of protecting the brain and forming the facial structure.
Cranial sutures and foramina are crucial for accommodating brain growth and facilitating the passage of nerves and blood vessels.
Common skull injuries can result from falls or collisions, leading to various complications, including contrecoup injuries and hematomas.
Overview of Skull Anatomy
The human skull is a complex structure composed of 22 bones, with 21 of them being fixed and one, the mandible, being movable. This bony structure can be divided into two main regions: the neurocranium and the viscerocranium. The neurocranium safeguards the brain, while the viscerocranium forms the facial skeleton. Together, they protect the brain, support facial muscles, and provide structural integrity to the face.
The facial skeleton protects sensory organs and frames facial tissues essential for eating and speaking. Additionally, the skull supports facial muscles and provides structural integrity to the face. Understanding skull anatomy is vital in clinical and surgical practices due to its complexity and the crucial structures it supports.
Several anatomical landmarks, such as the nasion, glabella, and bregma, are key points of reference for surgical and anthropological assessments. The upper part of the skull, known as the calvaria, protects essential components including the cerebral cortex and the eyes. The zygomatic bones contribute to the prominence of the cheeks and are essential for the aesthetic appearance of the face.
Human Skull Diagram
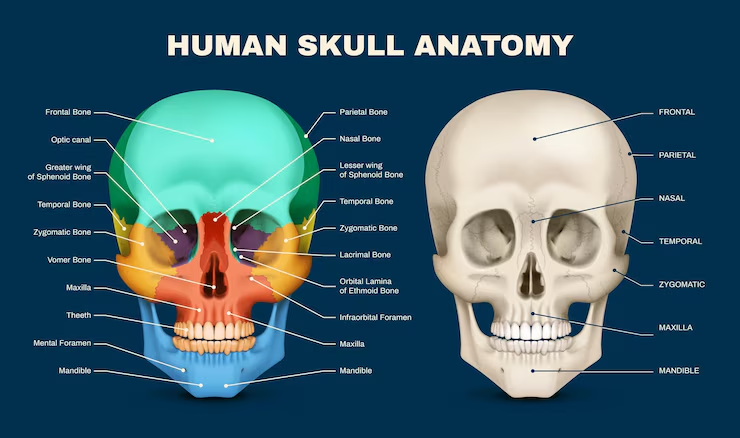
External Features of the Skull
The external bony structure of the skull serves as a protective casing for the brain and is composed of various interconnected bones. Key landmarks include the forehead region formed by the frontal bone, the parietal bones that form the top and sides, and the occipital bone at the back.
These bones not only protect the brain but also provide attachment points for muscles and serve as landmarks for medical professionals. The symmetry and integrity of these bones are crucial for both function and aesthetics.
Internal Structure of the Skull
The cranial cavity houses the brain, supported by various bones. This structure protects vital brain functions and allows the passage of nerves and blood vessels. The skull’s internal composition includes the neurocranium, encasing the brain, and the viscerocranium, forming the facial structure.
The upper part of the skull, known as the calvaria, protects the cerebral cortex and is composed of several bones. Foramina in the skull provide openings for the passage of cranial nerves and blood vessels, ensuring communication between the brain and the rest of the body.
Detailed Bone Analysis
This section explores the individual bones of the skull, each with unique features and functions that contribute to the overall structure and protection of the brain and sensory organs. It also covers cranial sutures, the fibrous joints connecting skull bones.
Cranial sutures, classified as synarthroses, permit no movement. In a fetal skull, these sutures are wider to allow slight movement during birth but become rigid over time.
Frontal Bone
The frontal bone consists of three main parts: squamous, orbital, and nasal. It starts as two halves that fuse during development. This bone articulates with several other bones including the parietal, zygomatic, sphenoid, ethmoid, lacrimal, maxillary, and nasal bones.
Its main function is to form the forehead and contribute to the formation of the upper eye sockets (orbits).
Parietal Bones
The parietal bones are located on the top and sides of the skull and are essential for the structural integrity of the cranium. These paired bones join at the top. The external surface features the parietal eminence near the center.
On the inner surface, features include the sulcus for the superior sagittal sinus and grooves for the middle meningeal artery. The superior and inferior temporal lines are associated with the attachment sites for the temporalis muscle.
Temporal Bones
The temporal bone is made up of several segments. These include the squamosal, mastoid, tympanic, styloid, and petrous portions. It articulates with the zygomatic, sphenoid, parietal, and occipital bones. The structures of the middle and inner ears are located within the petrous ridge. This bone houses critical neurovascular elements, including the lower seven cranial nerves and major vessels to/from the brain.
External features include the smooth squamous portion, zygomatic process, articular tubercle, and glenoid fossa. Inferior processes include the vaginal process and the styloid process.
Occipital Bone
The occipital bone features the foramen magnum, allowing the spinal cord to connect with the brain. It is located at the back and base of the cranium and comprises various features that provide protection for the brain.
This thick and curved structure is vital for cranial integrity.
Sphenoid Bone
The sphenoid bone is centrally located in the skull and connects with almost every other skull bone. It consists of a central body, two greater wings, and two lesser wings. The optic canals are located at the junction of the body and lesser wings. The greater wings form the anterior floor of the middle cranial fossa. The superior orbital fissure transmits several key structures including the oculomotor nerve and sphenoid bones.
The sella turcica is found in the midline of the middle cranial fossa. It provides support for the pituitary gland. The skull base, which includes the sphenoid bone, supports the bottom of the brain and houses the frontal lobe, temporal lobe, brain stem, and cerebellum.
Ethmoid Bone
The ethmoid bone is located between the nasal cavity and the orbits, playing a key role in nasal function and support. It contributes to the structure of the nasal cavity, providing necessary support for its function.
Key features include the crista galli and cribriform plates located in the anterior cranial fossa.
Other Skull Components
Besides the main skull bones, additional critical components include the auditory ossicles (malleus, incus, stapes) and the hyoid bone. These smaller bones are essential for hearing and supporting tongue and throat muscles.
Sutures of the Skull
A suture is an immobile joint between adjacent skull bones. The coronal and sagittal sutures, located at the top of the skull, play significant roles in structural integrity and accommodating brain growth during childhood by allowing the skull to expand.
The lambdoid suture terminates the sagittal suture at the posterior skull, connecting it to the occipital bone and the right and left parietal and temporal bones. Dense, fibrous connective tissue fills the gap between the bones at a suture. This tissue helps to join the bones together.
The asterion serves as a crucial reference point for skull measurements, marking the junction of several sutures.
Coronal Suture
The coronal suture connects the frontal bone to the parietal bones, running obliquely across the skull. It starts at the bregma, where it meets the sagittal suture, and extends down to the pterion. This suture is vital for accommodating brain growth during childhood. Closure of the coronal suture typically occurs around the age of 24 years.
Trauma to the area around the coronal suture can lead to serious injuries, including potential damage to the middle meningeal artery.
Sagittal Suture
The sagittal suture is a fibrous joint located between the two parietal bones, running from the anterior convergence with the coronal suture to the posterior convergence with the lambdoid suture. This suture is characterized by its interlocking, serrated appearance and is visible from both the superior and posterior perspectives of the skull.
The bregma is the junction where the sagittal and coronal sutures meet, marking a significant point in the anatomy of the neonatal skull. The lambda represents the intersection of the sagittal and lambdoid sutures, typically positioned at the center of the lambdoid suture and indicating the location of the posterior fontanelle in infants.
The sagittal suture is the final suture in the skull to fuse, usually completing this process around the age of 30.
Lambdoid Suture
The lambdoid suture is formed from dense connective tissue and is situated at the posterior part of the skull, linking the occipital bone with the parietal bones. Its name is derived from its resemblance to the Greek letter lambda (Λ), and it serves primarily to hold the bones together without any sensory or motor functions.
This suture is flexible during infancy to facilitate skull expansion as the brain grows. Closure of the lambdoid suture before brain development is complete can result in lambdoid synostosis, which may lead to abnormal skull shape. Lambdoid synostosis is one of the less common types of craniosynostosis, and it can cause asymmetry in the skull due to early fusion.
Squamous Sutures
The squamous suture connects the parietal bones, which form the upper sides of the skull, to the temporal bones that make up the sides and base. Sutures like the squamous suture are crucial for allowing the skull to adapt during childbirth and enable brain growth in infants.
Craniosynostosis can occur if the squamous suture fuses too early, leading to potential complications due to restricted brain growth. The squamous suture is sometimes referred to as the squamosal suture, highlighting its connection between the temporal and parietal bones.
This suture is prominently visible from a lateral perspective of the skull and extends from the pterion to the parietomastoid suture. Among the skull sutures, the squamous suture, along with the lambdoid suture, is one of the last to close, potentially remaining open until around the age of 60.
Metopic Suture
The metopic suture divides the two frontal bones located at the center of the forehead. Unlike other cranial sutures that fuse later in life, the metopic suture typically fuses during the first year, between 3 to 9 months of age. When it fuses, it can cause a thickening of the adjacent bone, resulting in a structure known as a metopic ridge.
Premature fusion of the metopic suture is referred to as metopic craniosynostosis, resulting in an abnormal head shape called trigonocephaly. This condition can lead to increased intracranial pressure if not treated, potentially causing developmental issues.
Fontanelles (in Infants)
Fontanelles are soft spots on a baby’s skull that later fuse into sutures. The anterior fontanelle is the largest and closes around 18-24 months of age. The posterior fontanelle is smaller and typically closes within the first two to three months. Sphenoidal and mastoid fontanelles are smaller, closing within six months.
These fontanelles allow the skull to expand with the growing brain and facilitate childbirth by making the skull more flexible.
Facial Skeleton
The facial skeleton is composed of 14 bones that form the structure of the face. These bones include paired bones such as the maxilla, palatine, zygomatic, nasal, lacrimal, and inferior nasal conchae, and unpaired bones like the vomer and mandible. The mandible is significant as the only movable bone of the skull and takes on a U-shape in adulthood, playing a crucial role in functions like eating, speaking, and facial expressions.
When there is an increase in tear production, some lacrimal fluid drains anteriorly, leading to a runny nose. These bones not only provide the structural framework for the face but also protect sensory organs and contribute to our appearance.
Maxillary Bones
The maxilla bones are involved in forming the upper jaw and play a critical role in the structure of the face. The hard palate is formed by the palatine processes of the maxilla and horizontal plates of palatine bones.
The infraorbital foramen serves as an exit point for a sensory nerve supplying the nose, upper lip, and anterior cheek.
Zygomatic Bones
Zygomatic bones, also known as cheekbones, form the lateral walls of the orbits and are located above the zygomatic arch. The muscles responsible for pulling the mandible upward during biting and chewing are linked to the zygomatic arch and the zygomatic bone. These muscles play a crucial role in the process of mastication.
These bones are crucial for the overall aesthetic appearance of the face.
Nasal Bones
The nasal bones are responsible for forming the upper structure of the nasal cavity and contribute significantly to the shape of the nose. These bones play a crucial role in defining the appearance of the nose and support facial aesthetics.
When the nose is broken, the nasal bones are damaged, which can affect both function and appearance.
Mandible
The mandible is recognized as the largest and most robust bone in the facial structure, shaped like a horseshoe. As the only movable bone in the skull, the mandible connects to the temporal bone at the temporomandibular joint, facilitating motion.
It consists of two primary parts: the body and the ramus, which extends upward on either side. This bone plays a critical role in mastication by anchoring the lower teeth and providing attachment points for several muscles involved in chewing.
Injuries to the mandible, such as fractures or dislocations, commonly occur due to trauma, impacting its function in chewing and speech.
Lacrimal Bones
The lacrimal bone, one of the smallest facial bones, is located in the medial wall of the orbit. It plays a key role in supporting the lacrimal apparatus, which is responsible for tear production. A vertical ridge on the lacrimal bone creates a depression that forms part of the nasolacrimal duct.
The lacrimal bone’s structure includes a hook-like projection that facilitates drainage of tears into the nasal cavity. Additionally, it serves as an attachment point for the orbicularis oculi muscle, aiding in eyelid closure.
Palatine Bones
The palatine bones are paired structures located between the maxillae and the pterygoid process of the sphenoid bone, contributing to the formation of the oral cavity, nasal cavity, and orbits. These bones have two main components: a horizontal plate forming part of the hard palate and a perpendicular plate that helps shape the lateral wall of the nasal cavity. They articulate with five other bones: the maxilla, sphenoid, ethmoid, inferior nasal concha, and vomer.
The horizontal plate constitutes the bony base of the posterior section of the hard palate and a portion of the floor of the nasal cavity. Unique processes include a pyramidal process that assists in forming the pterygoid fossa and an orbital process contributing to the orbital floor.
The greater palatine foramen, located in the horizontal plate, allows the passage of the greater palatine nerve and vessels.
Inferior Nasal Conchae
The inferior nasal concha is a unique, paired bone located on the lateral walls of the nasal cavity. This bone plays a vital role in filtering and humidifying inhaled air, contributing to respiratory health. Unlike the superior and middle nasal conchae, which are parts of the ethmoid bone, the inferior nasal concha stands as an independent structure.
It increases the surface area in the nasal cavity, aiding in air conditioning before it reaches the lungs. These bones are lined with mucous membranes that help trap debris and facilitate its movement towards the throat.
Vomer
The vomer is a thin, unpaired bone positioned vertically within the nasal cavity and is part of the facial skeleton. It contributes to the formation of the nasal septum along with the perpendicular plate of the ethmoid bone and nasal septal cartilage.
The vomer has two surfaces and four borders, including a superior border featuring a groove that accommodates the sphenoid bone. It articulates with four facial bones, specifically the maxillae and palatine bones, as well as two bones from the neurocranium, the sphenoid and ethmoid bones.
Unlike many other skull bones, the vomer’s posterior border does not articulate with any other bones.
Cranial Fossae
There are three distinct cranial fossae: the anterior, middle, and posterior, each formed by different cranial bones. These fossae are depressions in the skull base, each corresponding to different regions of the brain. The cranium consists of two parts: the cranial roof and the cranial base.
Each fossa plays a specific role in housing different parts of the brain and providing pathways for nerves and blood vessels. Understanding these structures is crucial for both anatomical studies and clinical practices.
Anterior Cranial Fossa
The anterior cranial fossa is primarily formed by the frontal bone and is the least deep among the cranial fossae. It contains the frontal lobes of the brain. Located most anteriorly and overlying the orbits, it is the shallowest of the three cranial fossae.
The floor of the anterior cranial fossa is mainly formed by the frontal bone.
Middle Cranial Fossa
The middle cranial fossa is situated behind the anterior cranial fossa. It occupies a distinct position within the cranial cavity. It houses the temporal lobes of the brain.
The bony prominence of the sella turcica divides the middle cranial fossa at the midline.
Posterior Cranial Fossa
The posterior cranial fossa houses the cerebellum and contains vital openings for the spinal cord and cranial nerves. The occipital bone forms the floor and posterior wall of this fossa.
Foramina and Fissures of the Skull
Foramina serve as openings in the skull that facilitate the passage of nerves and blood vessels. Fissures are narrow openings that allow connections between different anatomical structures. These openings are crucial for the proper functioning of the nervous and circulatory systems.
Understanding the location and function of these foramina and fissures is essential for medical professionals, especially in surgical procedures.
Foramen Magnum
The foramen magnum, meaning ‘great hole,’ allows the brainstem and spinal cord to connect. It is the largest opening in the skull, located at the base of the occipital bone. This opening serves as a crucial passage for the spinal cord, several arteries, and cranial nerve XI, which plays a role in neck movement.
Its position is vital for maintaining proper alignment between the skull and the cervical spine, aiding in upright posture. Anatomical variations in the shape and size of the foramen magnum can influence surgical access during procedures involving the brain and cervical spine.
Optic Foramen
Located in the lesser wing of the sphenoid bone, the optic foramen transmits the optic nerve and the ophthalmic artery. This foramen allows these structures to pass from the cranial cavity into the orbit, which are critical for vision. The optic foramen connects the orbit to the cranial cavity, and its development begins during the third month of gestation.
Clinical conditions affecting the optic nerve, such as optic neuritis and glaucoma, highlight the importance of the optic foramen in visual health.
Foramen Ovale
The foramen ovale allows the passage of the mandibular branch of the trigeminal nerve along with the accessory meningeal artery. It is located in the posterior section of the sphenoid bone. This foramen measures approximately 7.2 mm in adults and 3.85 mm in newborns.
In medical procedures, the foramen ovale serves as an entry point for treatments aimed at addressing trigeminal neuralgia. Failure to close the foramen ovale can result in a patent foramen ovale (PFO), which is a common congenital defect present in about 25% of the population.
Foramen Rotundum
This opening permits the maxillary division of the trigeminal nerve to enter the skull. The foramen rotundum is located in the sphenoid bone and connects the middle cranial fossa to the pterygopalatine fossa. It allows the maxillary nerve, a branch of the trigeminal nerve, to pass through.
The foramen rotundum’s shape evolves from oval to round during fetal development.
Foramen Spinosum
The foramen spinosum is a minor opening that allows the entry of the middle meningeal artery. This foramen, located in the greater wing of the sphenoid bone, allows the passage of the middle meningeal artery and vein. It serves as an important landmark in neurosurgery due to its proximity to other cranial foramina.
Variations in the foramen spinosum’s size and location are common.
Jugular Foramen
The jugular foramen is a key passage for three cranial nerves and the internal jugular vein, draining blood from the head. It is located at the base of the skull, formed by the temporal and occipital bones. Cranial nerves IX, X, and XI pass through the jugular foramen, enabling these nerves to connect to various structures outside the skull.
The jugular foramen is divided into two compartments: the pars nervosa and the pars vascularis.
Internal Acoustic Meatus
This passageway carries the facial and vestibulocochlear nerves, which are essential for hearing and balance. Located within the petrous part of the temporal bone, the internal acoustic meatus serves as a passageway between the posterior cranial fossa and the inner ear.
The canal typically measures around 1 cm in length and has smooth, rounded outer margins. The fundus of the internal acoustic meatus is divided by crests of bone, forming distinct areas for different nerve branches.
Supraorbital Foramen
The supraorbital foramen transmits the supraorbital nerve and artery, which supply the forehead and scalp. Located at the junction of the inner third and outer two-thirds of the superior orbital rim, it is crucial for the entry of the supraorbital nerve, a branch of the frontal nerve. The supraorbital artery also passes through this foramen to supply the frontal bone and surrounding areas.
In some individuals, the supraorbital foramen may be incomplete, in which case it is referred to as the supraorbital notch.
Infraorbital Foramen
This foramen allows the infraorbital nerve and vessels to reach the face. Located on the maxillary bone beneath the eye socket, it allows passage for the infraorbital artery, vein, and nerve. The distance from the infraorbital foramen to the infraorbital margin typically ranges from 6.10 to 10.9 mm.
This foramen serves as a pressure point for assessing the sensitivity of the infraorbital nerve.
Mental Foramen
The mental foramen transmits the mental nerve, which provides sensation to the chin and lower lip. Located on the outer surface of the mandible, it serves as a passage for the mental nerve and branches of the inferior alveolar artery and vein.
In a majority of individuals, the mental foramen aligns with the second premolar tooth. Variations in the number and location of mental foramina can occur.
Stylomastoid Foramen
The stylomastoid foramen allows the facial nerve to exit the skull and innervate facial muscles. Located between the styloid and mastoid processes, this foramen also allows passage for the stylomastoid artery, which supplies the facial nerve and surrounding structures.
Pterygoid Canal
The pterygoid canal, also known as the Vidian canal, is situated in the sphenoid bone and serves as a conduit for the Vidian artery and nerve, linking the middle cranial fossa to the pterygopalatine fossa. This canal facilitates the passage of the nerve of the pterygoid canal, contributing to the parasympathetic innervation of the glands.
It acts as a crucial anatomical landmark for locating the internal carotid artery as it exits from the petrous region of the temporal bone.
Fissures: Superior Orbital Fissure and Inferior Orbital Fissure
The superior orbital fissure is a significant triangular gap located at the back of the eye socket, positioned between the greater and lesser wings of the sphenoid bone. It transmits multiple cranial nerves that control eye movements and sensation, including the oculomotor, trochlear, and abducens nerves.
The inferior orbital fissure, located beneath the superior orbital fissure, connects with the pterygomaxillary fissure and allows the passage of the infraorbital nerve and vessels.
These fissures are crucial for the communication between the orbit and the cranial cavity, facilitating the transmission of nerves and blood supply.
Cavities of the Skull
The skull is designed with various cavities that house and protect essential structures like the brain, eyes, and respiratory system. These cavities include:
The cranial cavity
Orbital cavities
Nasal cavity
Oral cavity
These cavities play critical roles in protecting vital organs and facilitating their functions.
Cranial Cavity
The cranial cavity is enclosed by eight cranial bones, creating a protective environment for the brain. It is filled with cerebrospinal fluid, which enhances brain protection by filling spaces between the brain and meninges. This cavity houses the brain and its protective layers, ensuring the brain is shielded from physical impacts and infections.
Orbital Cavities
Each orbital cavity is primarily composed of seven different bones that collectively form the bony sockets for the eyes. These cavities house the eyeballs and are essential for eye movement and vision.
The orbital cavities also support associated structures such as extraocular muscles and nerves, which play crucial roles in the function and protection of the eyes.
Nasal Cavity
The nasal cavity is divided by the nasal septum and contains structures called conchae that help warm and humidify air. It houses the paranasal sinuses, which are air-filled spaces that reduce the weight of the skull and enhance voice resonance.
The nasal cavity is structured to warm, moisturize, and filter air before it enters the lungs, playing a vital role in respiratory health.
Oral Cavity
The oral cavity is formed by the maxilla and mandible, which support the teeth and facilitate chewing. It is crucial for mechanical digestion and plays a role in speech. The maxilla and mandible contribute to the upper and lower jaws, respectively, providing the structural framework for the oral functions.
Important Openings and Canals
Foramina and canals in the skull are essential for providing pathways for nerves and blood vessels, crucial for neurovascular functions. The jugular foramen serves as an exit point for cranial nerves and blood vessels, playing a vital role in the posterior cranial fossa. The foramen magnum is the largest opening in the skull, facilitating the passage of the spinal cord from the brain.
Other significant openings include the superior orbital fissure, which connects the orbit to the cranial cavity, allowing cranial nerves and the ophthalmic vein to pass. The internal acoustic meatus carries the facial and vestibulocochlear nerves, essential for hearing and balance. The carotid canal allows the internal carotid artery to reach the cranial cavity, supplying blood to the brain.
Skull Openings and Canal Diagram
Paranasal Sinuses
Paranasal sinuses are air-filled spaces located within the bones of the skull that play important roles in various craniofacial functions. These sinuses help reduce the overall weight of the skull and enhance the resonance of the voice.
The frontal bone contributes to the formation of the orbital cavity and houses the frontal sinuses. The maxillary sinuses are the largest paranasal sinuses and can be tricky to drain due to their high connection point to the nasal cavity.
Hyoid Bone
The hyoid bone is situated in the upper neck. It can be found close to the inferior mandible. It coordinates movements of the tongue, larynx, and pharynx, playing a crucial role in swallowing, speech, and breathing. This bone serves as an attachment point for several muscles, including those in the floor of the mouth and the larynx.
Common Skull Injuries
Skull injuries can range from minor fractures to severe traumatic brain injuries. Common types of skull injuries include linear skull fractures, which can radiate from the point of impact. Contrecoup injuries typically occur when a head in motion strikes a stationary object, causing damage opposite the impact site. Falls and vehicle collisions are the leading causes of contrecoup brain injuries.
In cases of contrecoup injuries, the extent of damage at the contrecoup site is often more severe than at the coup site. Some specific injuries include:
Epidural hematomas: These can sometimes appear on the opposite side of the skull from where the injury occurred.
Intracerebral hemorrhage: Present in 13 to 48% of adults with traumatic brain injuries.
Prognosis: The prognosis for contrecoup injuries varies widely based on the injury’s severity and associated conditions.


