

The knee is one of the largest and most complex joints in the human body. It plays a crucial role in movement, stability, and weight-bearing. Understanding the anatomy of the knee can help you better understand how to care for your knees and prevent injuries.
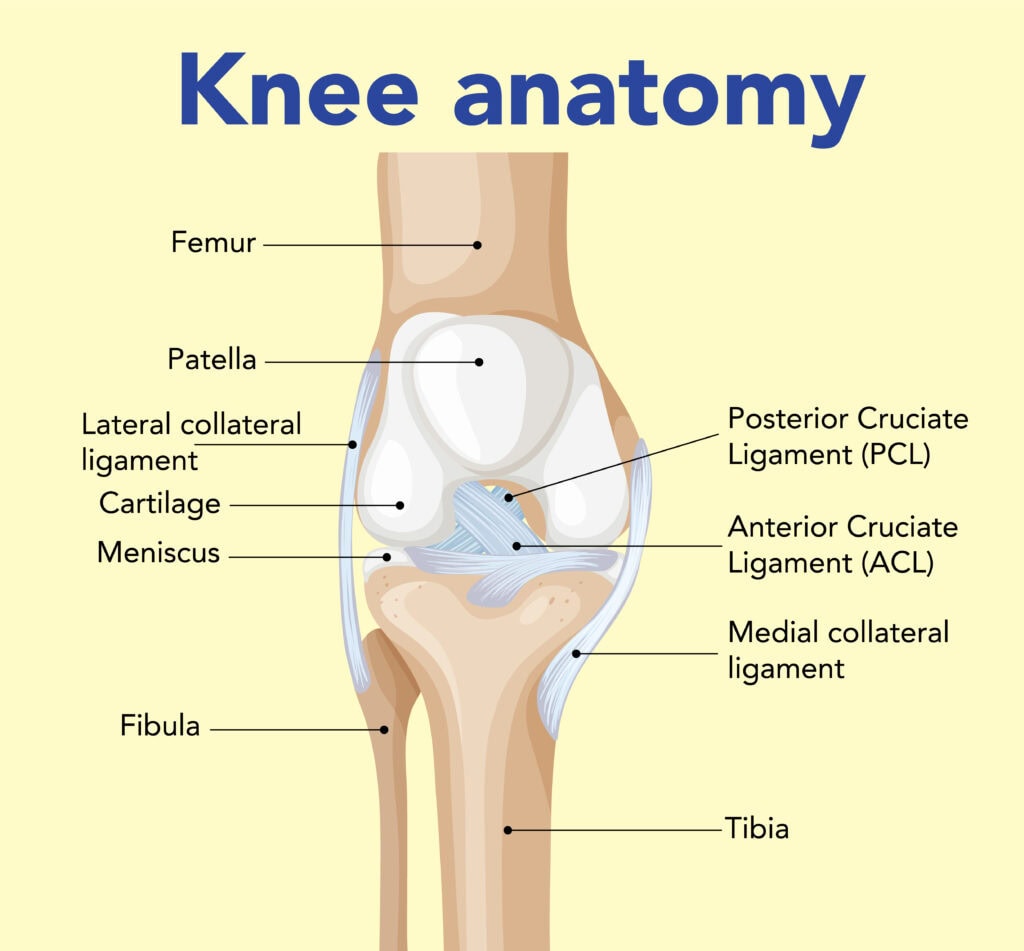
The knee joint is formed by three bones: the femur (thigh bone), tibia (shin bone), and patella (kneecap). The ends of these bones are covered with a smooth layer of cartilage which acts as a shock absorber and helps reduce friction during movement.
Ligaments, which are strong bands of tissue, connect the bones together. They provide stability to the knee joint and help prevent excessive movements that could cause injury.
Curious about knee anatomy? This guide explains the bones, ligaments, and movements that make your knee work.
Key Takeaways
The knee joint consists of three primary bones: the femur, tibia, and patella, each playing key roles in structure and movement.
Four main ligaments-ACL, PCL, MCL, and LCL-are essential for knee stability, limiting excessive movement and preventing injuries.
The knee’s functionality relies on various components including muscles, nerves, blood supply, and bursae, which work together to ensure smooth movement and stability.
Bones of the Knee Joint
The knee joint is a complex hinge joint involving three primary bones:
The femur, or thigh bone, connects with the tibia, commonly known as the shin bone, to form the main structure of the knee.
The tibia is the larger and stronger of the two bones in the lower leg.
The patella, or kneecap, sits in front of the knee joint, providing additional protection and aiding in movement.
Within the knee joint, the medial and lateral femoral condyle articulate with the corresponding tibial condyles, supporting weight-bearing activities. The tibial plateau, featuring two flattened condyles, is crucial for its articulation with the femur. The patellar groove facilitates smooth patella movement during knee flexion and extension, promoting efficient and pain-free motion.
Ligaments and Tendons
The knee joint contains four main ligaments:
Anterior cruciate ligament (ACL)
Posterior cruciate ligament (PCL)
Medial collateral ligament (MCL)
Lateral collateral ligament (LCL)
Ligaments and tendons are the unsung heroes of knee stability and movement. Each ligament is vital for maintaining knee stability.
The ACL frequently suffers injury from sudden twists or impacts, whereas the thicker PCL is less often injured. The MCL and LCL offer lateral and medial stability, preventing excessive side-to-side movement.
Tendons such as the quadriceps tendon and patellar tendon connect muscles to bones, facilitating movement and contributing to the overall stability of the knee joint.
Bones of the Knee
The knee joint comprises four main bones: the femur, tibia, patella, and fibula. Each of these bones plays a unique role in the structure and function of the knee, contributing to its strength, mobility, and stability.
1.1 Femur (Thigh Bone)
The femur is the longest and strongest bone in the human body, serving as the primary weight bearer in the thigh. It features two main condyles-the medial and lateral condyles-that articulate with the tibia and the menisci of the knee joint. These condyles are crucial for the smooth movement of the knee, allowing for both flexion and extension.
Smooth interaction between the femoral and tibial condyles ensures the knee can support significant weight while remaining flexible. This design enables the knee to perform a wide range of movements necessary for daily activities.
1.2 Tibia (Shin Bone)
The tibia, or shin bone, is the second largest bone in the body and serves as the main weight-bearing structure of the lower leg. Its structure includes the medial and lateral tibial plateaus, which form the surface for knee joint articulation. The tibial plateaus are covered by menisci, which help absorb shock and facilitate knee rotation, further enhancing the joint’s functionality.
The tibia’s design supports body weight and permits various movements. Its relationship with the femur and menisci maintains knee stability and flexibility, essential for walking, running, and jumping.
1.3 Patella (Kneecap)
The patella, or kneecap, shields the knee joint and boosts the quadriceps muscle’s leverage. Its articular surface ensures smooth movement during knee flexion and extension. Attached to the quadriceps tendon above and the patellar ligament below, the patella moves during knee flexion.
This sesamoid bone is crucial for the efficient functioning of the knee, contributing to the joint’s stability and movement. By acting as a fulcrum, the patella helps increase the force exerted by the quadriceps muscle, making movements like jumping and running more effective.
1.4 Fibula
The fibula is a slender bone located alongside the tibia, providing lateral stability to the knee but not bearing significant weight. Its upper end, known as the head of the fibula, connects to the knee joint and serves as a connection point for ligaments and tendons. The fibula contributes to the stability of both the knee and the ankle, playing a crucial role in overall leg function.
Though not a weight-bearing bone, the fibula is essential for maintaining the structural integrity of the knee, particularly during lateral movements. Its interactions with other bones and ligaments ensure that the knee can withstand various stresses and strains.
Knee Diagram
2. Joints of the Knee
The knee joint is classified as a modified hinge joint, allowing for flexion, extension, and a small degree of rotation. It consists of two primary joints: the tibiofemoral joint and the patellofemoral joint, which work together to facilitate knee movements. These joints are supported by a complex network of ligaments, tendons, and muscles that ensure the stability and functionality of the knee.
Grasping the structure and function of these joints helps appreciate the knee’s operation during various activities.
2.1 Tibiofemoral Joint
The tibiofemoral joint connects the medial and lateral condyles of the femur with the corresponding condyles of the tibia. This joint is the main weight-bearing component of the knee, playing a critical role in load-bearing and stability. The medial compartment of the tibiofemoral joint is crucial for load-bearing and stability, while the lateral compartment provides flexibility and movement.
The medial meniscus, shaped like a ‘C’, and the lateral meniscus, more ‘O’-shaped, reflect their differing anatomical structures and functions within the tibiofemoral joint. Together, they help absorb shock and distribute weight evenly across the knee.
2.2 Patellofemoral Joint
The patellofemoral joint is the area where the patella articulates with the femur. This joint serves to increase the leverage of the quadriceps muscle, reducing friction during knee movements and enhancing the efficiency of the knee joint.
The patellofemoral joint enables smooth patella movement over the femur, crucial for knee functionality during activities like running, jumping, and squatting. It also helps protect the knee joint from excessive wear and tear.
2.3 Superior Tibiofibular Joint
The superior tibiofibular joint connects the head of the fibula with the lateral aspect of the tibia. This joint allows for a degree of gliding movement between the tibia and fibula during knee flexion and ankle movements, contributing to the overall flexibility and stability of the knee.
Movement at the superior tibiofibular joint is essential for accommodating the dynamic demands placed on the knee during various activities. This joint plays a supporting role in ensuring the smooth and efficient functioning of the knee.
3. Ligaments of the Knee
The ligaments of the knee play a crucial role in stabilizing the joint and facilitating movement. The knee contains four primary ligaments that connect the femur to the tibia, each contributing to the knee’s overall stability and functionality.
3.1 Collateral Ligaments
The medial collateral ligament (MCL) and lateral collateral ligament (LCL) are the two main collateral ligaments in the knee. The MCL is positioned on the inner side of the knee and provides stability against lateral forces, while the LCL is found on the outer side of the knee and supports against medial forces. These ligaments help prevent excessive side-to-side movement, ensuring the stability of the knee during various activities.
Collateral ligaments preserve knee integrity, shielding it from sudden lateral impacts or twists. They are crucial for overall knee stability and function, including the tibial collateral ligament.
3.2 Cruciate Ligaments
The anterior cruciate ligament (ACL) and posterior cruciate ligament (PCL) are the two main cruciate ligaments in the knee. The ACL is crucial for controlling the forward movement and rotation of the tibia, preventing it from sliding too far forward relative to the femur. On the other hand, the PCL is responsible for controlling the backward movement of the tibia, helping to prevent it from sliding backward relative to the femur.
Cruciate ligaments are vital for knee stability, particularly during sudden directional changes or high-impact activities. They control the forward and backward movement of the knee, ensuring proper function.
3.3 Other Ligaments
In addition to the collateral and cruciate ligaments, the knee contains other important ligaments that contribute to its stability and function. The patellar ligament, a continuation of the quadriceps tendon, connects the kneecap to the tibia and is crucial for knee extension. The oblique popliteal ligament reinforces the back of the knee joint, providing additional stability during movement.
The arcuate popliteal ligament, located behind the knee, arches over the popliteus muscle and contributes to the knee’s stability during flexion. These ligaments work together to ensure the knee remains stable and functional during various activities.
4. Meniscus
The meniscus is crucial for shock absorption, load transmission, and joint stabilization in the knee. These fibrocartilaginous structures enhance joint stability, deepen the tibial plateau, and absorb shock during movement, ensuring the smooth and efficient functioning of the knee.
4.1 Medial Meniscus
The medial meniscus is larger than the lateral meniscus, measuring approximately 40.5-45.5 mm in length. It has a wedge shape that helps stabilize the femur during movement and covers about 50-60% of the knee’s articular surface, specifically between the medial femoral condyle and the tibial plateau. The medial meniscus is primarily supplied by the medial, lateral, and middle genicular arteries, which provide vascularity mainly to its outer sections.
This crescent-shaped structure plays a crucial role in stabilizing the knee and distributing weight evenly across the joint. Its shock absorption and stress reduction abilities are vital for joint health and functionality.
4.2 Lateral Meniscus
The lateral meniscus is more mobile than the medial meniscus and can adapt its shape during knee flexion. Generally smaller than the medial meniscus, with lengths averaging between 32.4-35.7 mm, the lateral meniscus is circular and covers more of the tibial articular surface. Its attachments are less firm compared to those of the medial meniscus, contributing to its increased mobility.
The lateral meniscus enhances knee flexibility and adaptability during movement. Its increased mobility allows it to accommodate the dynamic demands placed on the knee, ensuring smooth and efficient functioning during various activities.
5. Muscles of the Knee
The knee joint is supported by two major muscle groups: the hamstrings and the quadriceps. These muscles are essential for the knee’s movement and stability, particularly during activities such as walking and running.
5.1 Quadriceps Femoris
The quadriceps femoris group, comprising four muscles, works together to extend the knee joint: rectus femoris, vastus lateralis, vastus medialis, and vastus intermedius. The rectus femoris is unique among the quadriceps as it crosses both the hip and knee joints, allowing it to also flex the thigh. The vastus lateralis, located on the outer thigh, is one of the largest muscles in the quadriceps group, while the vastus medialis, often referred to as the teardrop muscle, plays a crucial role in stabilizing the knee joint.
These muscles are vital for the efficient functioning of the knee, enabling movements such as walking, running, and jumping. The quadriceps femoris group works in harmony to ensure the knee can perform a wide range of activities.
5.2 Hamstrings
The hamstrings are a group of three muscles located at the back of the thigh that primarily function to flex the knee. These muscles include the biceps femoris, semitendinosus, and semimembranosus. The biceps femoris has two heads and is involved in both knee flexion and hip extension, while the semitendinosus assists in the flexion of the knee and contributes to the rotation of the leg when the knee is bent.
The semimembranosus helps stabilize the knee and supports hip extension, ensuring the smooth and efficient functioning of the knee during various activities. The hamstring muscles are essential for maintaining knee stability and flexibility.
5.3 Other Muscles
In addition to the quadriceps and hamstrings, other muscles also play a significant role in knee function. The popliteus muscle, located at the back of the knee, plays a key role in unlocking the knee from a fully extended position, enabling flexion. The gastrocnemius muscle, part of the calf, crosses the knee and assists in bending the knee.
These muscles ensure the knee can perform a wide range of movements, contributing to overall joint stability and functionality. Their importance in maintaining knee health and preventing injuries cannot be overstated.
6. Nerves of the Knee
The knee contains several important nerves, including the femoral nerve, tibial nerve, common peroneal nerve, and saphenous nerve, which facilitate movement and sensation. These nerves are essential for maintaining the knee’s functionality and ensuring proper coordination during activities.
6.1 Tibial Nerve
The tibial nerve is responsible for innervating muscles in the back of the leg, which are crucial for movements such as plantar flexion of the foot. This nerve branches off from the sciatic nerve and innervates the posterior compartment of the leg, affecting muscles responsible for knee flexion and ankle movement.
The tibial nerve plays a vital role in ensuring the smooth and efficient functioning of the knee, contributing to its overall stability and flexibility. Its importance in maintaining proper movement and sensation in the leg cannot be overstated.
6.2 Common Peroneal Nerve
The common peroneal nerve plays a significant role in innervating the muscles that allow for dorsiflexion and eversion of the foot. This nerve wraps around the neck of the fibula and primarily supplies the muscles of the lateral compartment of the leg, enabling foot dorsiflexion and eversion.
The common peroneal nerve is essential for the proper functioning of the knee, contributing to its overall stability and flexibility. Its role in facilitating movement and sensation in the leg is crucial for maintaining knee health.
6.3 Saphenous Nerve
The saphenous nerve, the longest branch of the femoral nerve, provides sensory innervation to the medial leg and foot. It plays a vital role in sensory feedback, ensuring proper coordination and movement.
The saphenous nerve is essential for maintaining the sensation and functionality of the knee, contributing to its overall stability and flexibility. Its importance in ensuring proper sensory feedback and movement cannot be overstated.
7. Blood Supply of the Knee
The blood supply to the knee originates from several major arteries that create a network of anastomoses around the joint. This network ensures the knee receives the necessary nutrients and oxygen to maintain its health and functionality.
7.1 Popliteal Artery
The popliteal artery is a continuation of the superficial femoral artery and bifurcates into the anterior tibial artery and the common trunk of the posterior tibial and peroneal arteries. It branches into five primary arteries that supply blood to different areas of the knee, ensuring the joint receives the necessary nutrients and oxygen to function properly.
The popliteal artery is vital for knee health, contributing to overall stability and flexibility. Its importance in providing blood supply to the knee cannot be overstated.
7.2 Genicular Anastomosis
The genicular anastomosis consists of arteries that interconnect to facilitate blood flow to the knee joint during movement. This network includes the superior medial, superior lateral, inferior medial, and inferior lateral genicular arteries, each providing essential blood supply to different areas of the knee.
These arteries provide essential nutrients and oxygen to the knee, crucial for maintaining joint stability and flexibility during movement.
7.3 Veins of the Knee
The popliteal vein, running alongside the popliteal artery, drains blood from the knee and lower leg, ensuring the joint receives essential nutrients and oxygen.
The great saphenous vein drains superficial structures around the knee, contributing to joint health and functionality.
8. Bursae of the Knee
Bursae are small, fluid-filled sacs that help reduce friction in the knee joint. These structures serve as cushioning mechanisms, allowing for smooth movement and reducing stress on the knee during various activities.
8.1 Suprapatellar Bursa
The suprapatellar bursa is located above the kneecap and acts as a cushion between the femur and the quadriceps tendon. This bursa is situated above the kneecap, positioned between the femur and the quadriceps tendon, ensuring the smooth movement of the knee during various activities.
The suprapatellar bursa reduces friction and cushions the knee, contributing to overall stability and functionality.
8.2 Prepatellar Bursa
The prepatellar bursa is situated in front of the kneecap, providing protection and reducing friction during movement. Located in front of the kneecap, this bursa acts as a cushion between the skin and the patella, ensuring the smooth movement of the knee during various activities.
The prepatellar bursa reduces friction and cushions the knee, contributing to overall stability and functionality.
8.3 Infrapatellar Bursa
The infrapatellar bursa is divided into two parts: the subcutaneous infrapatellar bursa and the deep infrapatellar bursa. The subcutaneous infrapatellar bursa lies beneath the skin in front of the kneecap, cushioning it against pressure, while the deep infrapatellar bursa is found deeper in the knee, between the patellar tendon and the tibia.
These bursae reduce friction and cushion the knee, contributing to overall stability and functionality.
8.4 Other Bursae
In addition to the suprapatellar, prepatellar, and infrapatellar bursae, the knee contains other important bursae such as the pes anserine bursa and the semimembranosus bursa. The pes anserine bursa is located on the inner side of the knee and helps reduce friction between tendons and bones, providing cushion to the tendons of the hamstrings.
The semimembranosus bursa is positioned near the semimembranosus muscle, cushioning it as it moves. This bursa is located between the semimembranosus tendon and the femur, helping to reduce friction during knee movement.
9. Clinical Considerations
A thorough understanding of knee anatomy is crucial for diagnosing and treating various knee conditions, including common injuries, degenerative conditions, and utilizing diagnostic techniques.
9.1 Common Injuries
Common knee injuries include:
ACL tears, which are prevalent in athletes participating in sports that involve pivoting or abrupt stops, often identified by a ‘pop’ sound and immediate swelling.
Meniscal tears, which can occur due to twisting motions or heavy lifting.
Patellar dislocations, which usually happen from a direct blow to the knee or a sudden change in direction, potentially leading to a knee injury.
MCL injuries usually occur from direct blows to the outer knee, leading to pain and tenderness on the inner side, with bracing often recommended for treatment.
Meniscal tears can cause pain and locking sensations in the knee and may heal without surgical intervention depending on their severity. Prompt treatment of knee injuries prevents complications and supports proper recovery.
9.2 Degenerative Conditions
Degenerative conditions affecting the knee include osteoarthritis and rheumatoid arthritis. Osteoarthritis in the knee can develop following ACL injuries, especially if not managed properly, leading to chronic pain and functional limitations.
Rheumatoid arthritis is another degenerative condition that can affect the knee, causing inflammation and damage to the joint. Comprehending these conditions aids in developing effective treatment plans and maintaining knee health.
9.3 Diagnostic Techniques
Diagnostic techniques for knee issues include MRI, X-ray, and arthroscopy. MRI is the preferred imaging method for diagnosing ACL injuries due to its high sensitivity and specificity, allowing for detailed visualization of soft tissues. X-rays are useful for assessing bone structures and detecting fractures or degenerative changes.
Arthroscopy is a minimally invasive procedure that allows for direct visualization and treatment of knee problems using a small camera. These diagnostic techniques are essential for accurately diagnosing knee conditions and developing effective treatment plans.
10. Surgical Interventions
Surgical interventions for knee issues can significantly improve joint function and reduce pain. These interventions vary based on the specific ligament affected and the severity of the injury.
10.1 Arthroscopic Surgery
Arthroscopic surgery is a minimally invasive procedure that allows surgeons to visualize and treat knee problems using a camera. Meniscectomy involves the removal of a damaged meniscus to alleviate symptoms and restore function. ACL reconstruction typically involves using a graft from the patient’s own tissue or a donor to replace the torn ligament.
This procedure allows for repairs through small incisions, reducing recovery time and minimizing complications. Arthroscopic surgery is a valuable tool for treating various knee conditions and improving patient outcomes.
10.2 Total Knee Replacement
Total knee replacement is indicated for patients with severe arthritis or significant knee damage that compromises mobility. The procedure involves removing damaged cartilage and bone, followed by the insertion of a prosthetic joint. This surgery is commonly indicated for severe arthritis and significant knee damage that affects mobility.
During a total knee replacement, the damaged joint surfaces are removed and replaced with artificial components, significantly improving joint function and reducing pain. This procedure is essential for patients with advanced knee conditions, providing them with improved quality of life.
10.3 Osteotomy
Osteotomy is a surgical procedure that involves cutting and reshaping the bones to relieve pressure on the knee joint. High tibial osteotomy is performed to relieve pressure on the medial compartment of the knee by realigning the tibia, while distal femoral osteotomy is done to correct angular deformities in the knee by adjusting the femur.
These procedures redistribute weight and relieve pain, improving overall knee function. Osteotomy enhances mobility and quality of life for patients with specific knee conditions.
Menisci and Cartilage
The menisci and cartilage in the knee play crucial roles in absorbing shocks and reducing stress on the joint during movement. The medial meniscus and lateral meniscus possess a complex collagen structure that allows them to endure multidirectional stresses from normal knee activities.
Articular cartilage covers the surfaces of the femur, tibia, and patella, minimizing friction during joint movement. The presence of hyaline cartilage is crucial for maintaining the overall health of the knee, preventing degenerative changes over time. These structures are essential for the smooth and efficient functioning of the knee.
Muscles Surrounding the Knee
The quadriceps femoris group includes four muscles: vastus medialis, vastus lateralis, vastus intermedius, and rectus femoris, primarily responsible for knee extension, essential for walking and sitting.
The popliteus muscle is crucial for unlocking the knee joint from a fully extended position, enabling flexion. Together, these muscles play a vital role in enabling smooth and efficient movements of the knee joint during various physical activities.
Common Knee Injuries
ACL injuries often occur in non-contact sports, characterized by a ‘pop’ sound and immediate swelling. MCL injuries, usually from direct blows to the outer knee, cause inner knee pain and tenderness, often treated with bracing.
Meniscal tears can cause pain, locking sensations in the knee, and may heal without surgical intervention depending on their severity. Prompt treatment of knee injuries prevents complications and supports proper recovery.
Physiological Variants and Conditions
Physiological variants and conditions affecting the knee include genu varum and genu valgum, characterized by bowed legs and knocked knees. Mild-to-moderate cases can be treated with knee bracing, while severe cases may require surgery. Ehlers-Danlos syndrome can cause knee ligamentous laxity, affecting the stability and functionality of the knee, while vitamin D deficiency can lead to osteomalacia, presenting with bowleggedness.
Skeletal dysplasia is a rare congenital condition that may affect the knee, leading to various structural abnormalities. Comprehending these conditions aids in developing effective treatment plans and maintaining knee health.
Surgical Interventions
Surgical interventions for knee issues include:
Total knee arthroplasty, which replaces damaged components with metal, ceramic, or plastic prosthetics, improving joint function and reducing pain
Arthroscopy, which treats knee problems with a small camera and instruments through tiny incisions, minimizing recovery time
Ligament repair
Meniscectomy
Ligament repair and meniscectomy treat ligament tears and meniscal injuries, respectively, essential for restoring knee function and improving patient outcomes.
Other Considerations
Other considerations for knee health include bursae, the synovial membrane, and blood supply. Bursae are fluid-filled sacs that reduce friction and cushion the knee during movement. The synovial membrane produces synovial fluid, lubricating the knee joint and nourishing cartilage.
The middle genicular artery supplies the cruciate ligaments and synovial membrane, ensuring the knee receives essential nutrients and oxygen. These factors are crucial for understanding knee health and efficiency.
Frequently Asked Questions
What are the main bones involved in the knee joint?
The main bones in your knee joint are the femur, tibia, and patella, with the fibula providing some support too. So, next time you think about your knee, remember these key players!
What is the function of the menisci in the knee?
The menisci are crucial for your knee health as they absorb shock, distribute weight evenly, and improve joint stability. Keeping them healthy is key to maintaining good mobility.
What are common knee injuries?
Common knee injuries like ACL tears, meniscal tears, and patellar dislocations can really sideline you, so it’s essential to get them treated quickly to avoid further issues. Don’t let a knee injury hold you back!
How does the blood supply to the knee work?
The blood supply to the knee primarily comes from the popliteal artery and its branches, providing essential nutrients and oxygen. This rich vascular network is crucial for knee health and function.
What are some surgical interventions for knee issues?
Surgical options for knee issues like arthroscopic surgery, total knee replacement, and osteotomy can really enhance joint function and ease pain. If you’re facing knee trouble, these procedures could be worth considering.



